The Statement
A social media post claims the World Health Organization (WHO) released guidance that included an admission PCR tests for COVID-19 were producing inaccurate results due to earlier testing approaches.
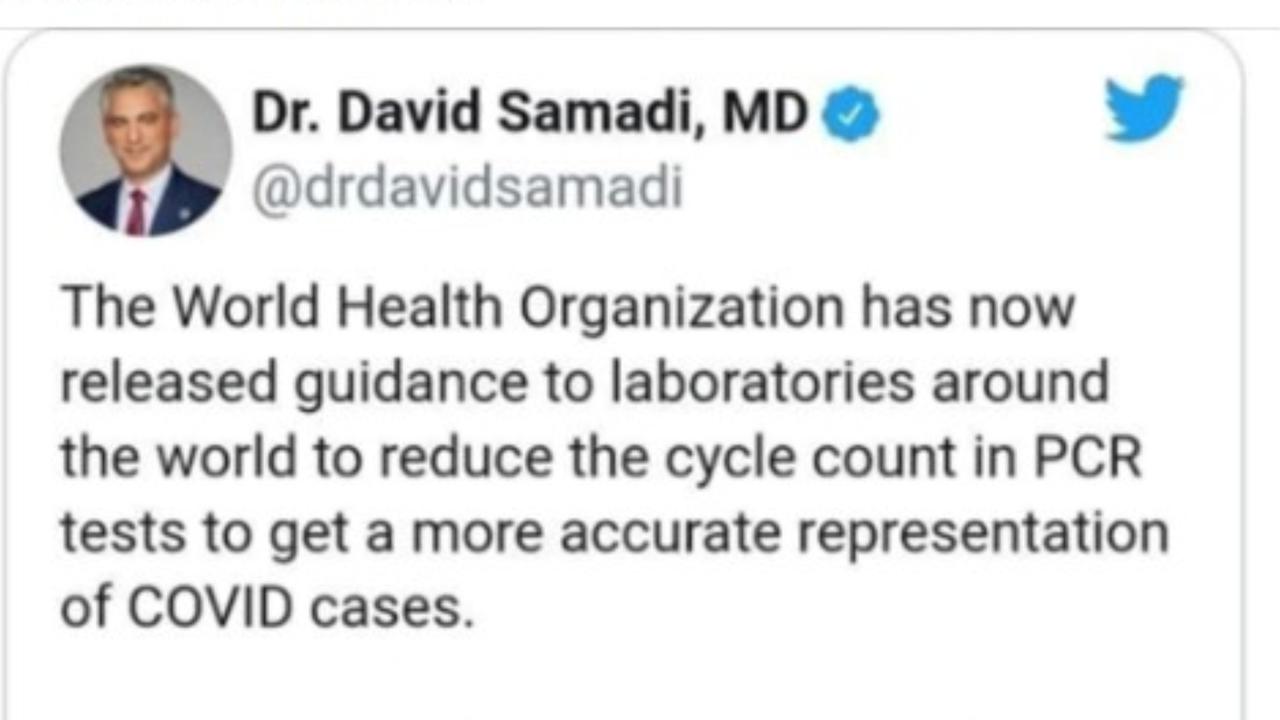
The Facebook post by a New Zealand user, who described herself as a "TV medium and healer", includes a screenshot of a January 21 tweet which reads: "The World Health Organization has now released guidance to laboratories around the world to reduce the cycle count in PCR tests to get a more accurate representation of COVID cases. The current cycle was much too high and resulting in any particle being declared a positive case."
At the time of writing, the January 23 post had generated more than 140 shares, 160 reactions and 15,000 views.
The Analysis
The tweet in the Facebook post wrongly claims that the WHO told laboratories to "reduce the cycle count" of PCR tests because current methods were leading to false positive results. In fact, the WHO notice called for "careful interpretation" of weak positive results but included no advice about reducing cycles.
The original tweet, from urologist and Newsmax pundit David Samadi, no longer appears on Twitter, however multiple screenshots of the post have been shared elsewhere on social media (see example here).
The term "cycle counts" refers to the cycle threshold (Ct) used in PCR tests. This represents the number of times a sample has been amplified before a positive case is detected in a laboratory.
A low Ct value indicates the sample being tested contains a high concentration of viral material, typically linked to a high risk that a person is infectious, according to a Public Health England guide. High values point to low viral concentrations and infectivity - although this may not be true in cases that were detected early.
A high Ct value does not indicate that a false positive has been generated - only that a low viral load is present in the patient.
The WHO guidance from January 20 addressed instances of diagnostic testing where weak positive results occurred and "where test results do not correspond with the clinical presentation".
It included a note that the "cycle threshold (Ct) needed to detect virus is inversely proportional to the patient's viral load" but contained no other references to test cycles other than advice that testers provide Ct values in their reports to health providers.
Joshua Freeman, who is clinical director of microbiology at Canterbury District Health Board, told AAP FactCheck via email: "The notice from the WHO was a reminder to laboratories using commercial PCR tests to follow the manufacturer's instructions for use.
"In particular the WHO highlights in this notice that weak positive results (high Ct values) in low prevalence settings need to be interpreted cautiously."
The WHO guidance includes a warning to PCR test users that "as disease prevalence decreases, the risk of false positives increases". Disease prevalence is the share of the overall population infected with the virus.
Dr Freeman said the WHO "did not make a blanket recommendation to 'reduce the cycle count'" as claimed in the tweet.
"Rather, the WHO advised reporting of Ct values to the requesting health care provider as an aid to interpretation and most importantly adherence to the manufacturer's instructions for use," he said.
Dr Freeman added there was "no evidence" to support the second claim suggesting tests that used high Ct cycles were returning large numbers of false positives.
"If anything, the bigger issue described in the scientific literature has been false negative results, primarily in patients presenting to hospital with severe respiratory illness," he said.
AAP FactCheck previously debunked claims that PCR tests were delivering high numbers of false positives and that this was rendering reported case numbers meaningless. A Public Health Ontario analysis of test results, published in September, found a false positive rate of less than 0.01 per cent, although it noted the risk of false positives increased where prevalence was low.
Alexander Khromykh, an associate professor of virology at the University of Queensland, told AAP FactCheck one of the factors that could contribute to interpretation of the PCR test was its timing.
"As virus infection is a dynamic process, low PCR positivity (high Ct values) early in infection can become high PCR positivity (low CT values) later in infection," Dr Khromykh said.
"Clinical presentation therefore would be another measure that needs to be considered for the timing when to perform the test."
He pointed to another line in the WHO guidance that touched on this point. It advised: "Where test results do not correspond with the clinical presentation, a new specimen should be taken and retested using the same or different NAT technology."
Professor Michael Baker, an epidemiologist with the Department of Public Health at the University of Otago, said the tweet was "misinformation" that did not accurately represent the content of the WHO communication.
"The WHO notification is reminding people that you have to interpret the testing results in the context in which the specimen is collected," he said during a phone interview with AAP FactCheck.
"The high Ct value may correspond to someone who's had historic infection and is no longer infectious, for instance. So I think it would be good practice to start recording that information so that we'll get a better understanding as to whether it corresponds, in any way, to someone's level of infectivity."

The Verdict
The tweet included in the post makes two false claims about the WHO's guidance on PCR tests.
The guidance does not advise laboratories to reduce the "cycle count" to improve the accuracy of PCR test, nor does it identify that current approaches were leading to a high number of false positives. Rather, it reminds test users to undertake "careful interpretation" of weak positive results and to adhere to manufacturer's instructions. Experts say properly conducted PCR tests return only a very small number of false positive results for COVID-19.
False - Content that has no basis in fact.
AAP FactCheck is an accredited member of the International Fact-Checking Network. If you would like to support our independent, fact-based journalism, you can make a contribution to AAP here.